Sex development, puberty, and transgender identity
Reproductive Biology for for Politicians and Voters, Part 2A

Transgender-related issues have recently received a great deal of attention in political discourse, resulting in polarization and controversy.
As a reproductive biologist, I find it frustrating when people (on both sides!) make mistakes resulting from a lack of understanding of the biology behind these issues. For example, pro-transgender people often dismiss the differences in athletic capabilities between cisgender and transgender women, and anti-transgender people often confuse puberty blockers with cross-sex hormones.
So in order to help people make better informed decisions, I will provide a biological overview of the following topics:
Definition of terms, including intersex and transgender
Basic developmental biology of sex
Prevalence and potential causes of transgender identity
As with my previous post, I will attempt to remain as neutral as possible, and stick to scientific facts instead of my personal opinions. And where the science isn’t fully settled yet, I will be sure to point this out, instead of confidently proclaiming something which might be wrong.
Given the length of this post so far, I’m splitting the second half into a separate post. Part 2B will focus on:
How puberty blockers work and their potential for side effects
Effects of cross-sex hormone therapy and other transgender medical procedures
Athletic performance of transgender women vs. cisgender women
Definition of terms
Sex: A biological trait, based on the production of male gametes (sperm) or female gametes (eggs).
Disorders of sex development (also known as differences of sex development)1: Developmental abnormalities affecting sex characteristics.
Intersex: People who have sex characteristics that are not fully male or fully female, due to disorders of sex development.
Gender: A social trait, based on identification as a man or woman (or occasionally a third gender).
Cisgender: People who have gender matching their sex.
Transgender men: People who have female sex (also known as “assigned female at birth”) and male gender.
Transgender women: People who have male sex (also known as “assigned male at birth”) and female gender.
Gender nonbinary: People (of either sex) who do not identify with either male or female gender.2
Gender dysphoria: Psychological distress resulting from a mismatch between a person’s gender identity and sex.
Gender-affirming care: A broad term that can refer to a variety of medical treatments aiming to reduce gender dysphoria, including puberty blockers, hormone therapies, and surgeries.
Puberty blocker: Medication that prevents the production of sex hormones (thus preventing puberty).
Masculinizing hormone therapy: Medication that increases levels of male sex hormones and decreases levels of female sex hormones.
Feminizing hormone therapy: Medication that increases levels of female sex hormones and decreases levels of male sex hormones.
Gender-affirming surgery (also known as “sex reassignment surgery”): A variety of surgical procedures, intended to take the anatomical structures present in one sex, and change them to become more similar to the structures present in the opposite sex.
Let’s talk about sex
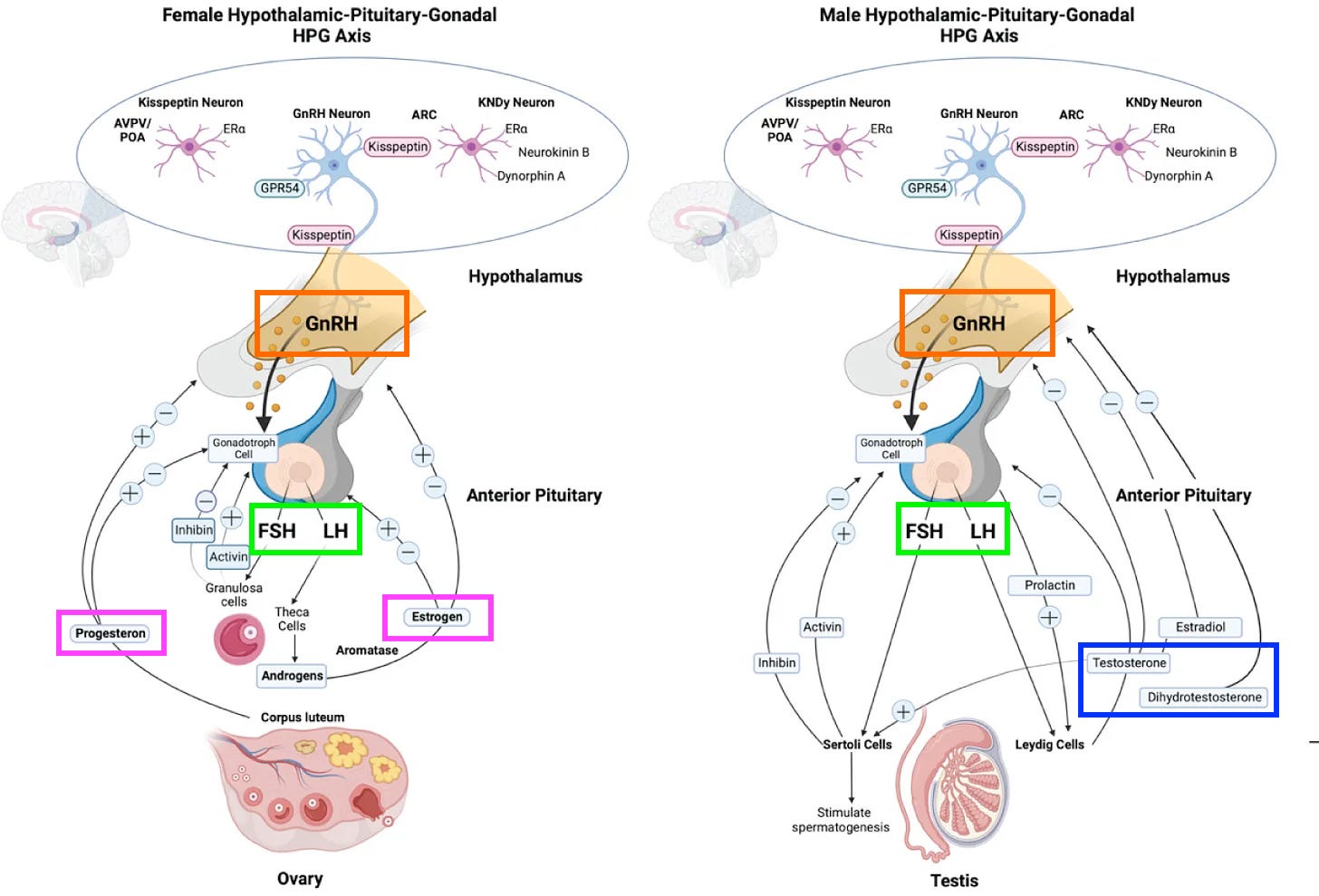
In mammals, sex is determined by the presence of a Y chromosome. Individuals with Y chromosomes are genetically male and individuals without Y chromosomes are genetically female. During fetal development, the SRY gene on the Y chromosome directs the gonads to develop into testes instead of ovaries. Testes and ovaries are different in their primary sex characteristics: testes make sperm and ovaries make eggs. Additionally, testes and ovaries produce different levels of sex hormones. Ovaries produce high levels of estrogen and progesterone, and low levels of testosterone, whereas testes produce moderate levels of estrogen and progesterone, and high levels of testosterone.3 These hormones cause secondary sex characteristics to develop throughout the rest of the body. For example, estrogen causes breasts to grow, and testosterone causes body hair to become thicker.
The production of sex hormones is regulated through the hypothalamic-pituitary-gonadal (HPG) axis. Puberty begins when the hypothalamus starts to secrete pulses of the hormone GnRH to the pituitary gland.4 In response, the pituitary secretes hormones (FSH and LH) which travel through the blood and act to increase the production of hormones (including progesterone, estrogen, and testosterone) by the testes and ovaries. These hormones5 act in a feedback loop6 to control the rate of GnRH, FSH, and LH release.
Beginning during fetal development and sharply increasing during puberty, the ovaries or testes produce sex hormones (estrogen for both males and females, and testosterone for males), which regulate important processes such as bone development, muscle growth, and brain development. This results in males and females having biological differences in traits such as basal metabolic rate, grip strength, and maximal respiratory rate.
Notably, male and female brains are different. Even before puberty, sex is evident just from an MRI brain scan. Some traits, such as the structure of a particular region of the hypothalamus known as the sexually dimorphic nucleus, show clear distinctions between males and females. Other traits show more overlap between the sexes, although still with some differences.

Disorders of sex development occur in about 1 in 5,000 people, usually due to genetic mutations. These include:
Gonads fail to develop. This can happen in both XY and XX individuals for a variety of reasons. No sex hormones are produced, and sex characteristics are mostly female but puberty does not occur.
SRY deletion: an XY individual develops ovaries and female characteristics.7
5α-reductase deficiency: an XY individual develops testes, but does not produce enough of the highly active form of testosterone. Sex characteristics can be ambiguous. However, testosterone production increases during puberty, often leading to the development of male characteristics later in life.
Androgen insensitivity: an XY individual develops testes which produce testosterone, but the body cannot respond to testosterone and develops female secondary sex characteristics.
Congenital adrenal hyperplasia: the adrenal glands produce excess testosterone.8 In XX individuals this can result in the development of some male characteristics (with the degree depending on the testosterone levels).
Kallmann syndrome: the pituitary does not receive GnRH,9 meaning sex hormone levels are low and puberty does not occur.
Sex chromosome aneuploidies (X0, XXY, etc.) also affect sex development, but male or female characteristics still follow the presence or absence of a Y chromosome.
Intersex individuals are people with biological sex characteristics that are not within the normal male or normal female developmental ranges. This is relatively rare, occurring in approximately 1 in every 2000 to 4500 people.10 Notably, most transgender people are not intersex.
Prevalence and potential causes of transgender identity
Statistics on the prevalence of transgender identity rely on self-identification through surveys, and may be unreliable due to people not wanting to disclose their transgender identity, or due to cisgender people giving spurious responses. Here, I will look at sources which analyze data from the CDC’s Behavioral Risk Factor Surveillance Survey, which is a relatively high-quality yearly phone-based survey from the United States. With that disclaimer out of the way, let’s look at the survey results:
In the United States as of 2017-2019 (the most recent range for which complete data are available for youth ages 13-17), 0.5% of the adult population (~1.3 million) and 1.4% of youth ages 13 to 17 (~0.3 million) identify as transgender. There are slightly more transgender women than transgender men.11 Although rates are roughly similar among different racial groups,12 they vary by geographical location, with a 4 to 5-fold difference among the states with the highest and lowest rates.13 In the 5 years leading up to the 2017-2019 survey period, the overall rates remained stable over time.
Looking at data from more recent years (2020-2023), the prevalence of transgender identity has sharply increased among young adults aged 18-24.14 This increase has largely been driven by individuals of female sex identifying as nonconforming/nonbinary or as transgender men, and the increase has taken place in different states of the USA at similar rates, regardless of whether the states were politically liberal or conservative.

The causes of transgender identity (and its recent increase) are a topic of intense debate. There is not currently a clear answer, and it is likely that multiple factors contribute. Potential causes can be divided into two categories: biological and social.
Genetics are an important component of many human behavioral traits, but mainly due to political difficulties as well as its low prevalence, there have not been any large-scale genome wide association studies of of transgender identity. Smaller studies examining correlations between different types of twins15 have estimated the genetic heritability,16 and found results ranging from 0% to 84% with most studies in the 30-60% range. For comparison, the heritability of homosexual behavior was recently estimated in a large, high-quality study as as 8 to 25%. Overall, I expect there to be some genetic component to transgender identity, but genetics are only one of many contributing factors.
Environmental factors may also play a biological role. These include things like endocrine-disrupting chemicals,17 hormone levels during fetal development, or just random variation in brain development.
In terms of brain structure, pre-treatment transgender individuals typically match their biological sex, but more research is needed in this area to uncover potential associations between brain structure and gender identity. One study from 2009 examined the brain structures of 24 transgender women prior to feminizing hormone treatment, comparing them to 30 control cisgender men and 30 control cisgender women. The transgender women had brains that generally matched their male biological sex. One brain region looked more similar to female brains, but given the relatively small sample size it is hard to draw definitive conclusions from this study. A 2015 imaging study of adolescents (55 transgender boys, 38 transgender girls, 44 cisgender boys, and 52 cisgender girls) found that brain structure largely followed biological sex, with only “subtle deviations” in transgender individuals. Overall, high-quality studies in this area are lacking, especially given that thousands of participants are typically required to draw reliable conclusions about associations between brain structure and traits,
Given that biological parameters (genetics and the developmental environment) have not changed much over the last decade, it seems likely that social causes are behind the recent rise in transgender identity. For example, greater societal acceptance of transgender identity could cause more transgender people to “come out” as transgender.18 Likewise, if transgender identity is viewed as desirable among certain social groups (such as young people), this might induce more of them to identify as transgender, continuing a social trend.19 Or, if cisgender people enforce rigid expectations of gender identity, people who don’t fully conform to them might identify as gender nonbinary. There is not much concrete evidence here, but one or more social causes are likely important.
After looking at the evidence, I think the following combined biological and social model (inspired by the liability threshold model of genetics) may be a good way of thinking about the causes of transgender identity, although this is highly speculative:
Every individual has a different innate propensity for gender-nonconforming identity and behavior. This propensity is largely biological. When the propensity is above a certain threshold, the person will identify as transgender.
This threshold at which someone identifies as “transgender” or “gender nonbinary” is largely socially determined, and has changed in recent years.
Again, I want to emphasize that the causes of transgender identity are still an area of active research and heated debate. Hopefully scientists will learn more over the coming years about this.
Stay tuned for the next part of this post, covering transgender medical treatments and athletics.
Whether something is a difference or disorder depends on whether it negatively affects the individual who has it. As most of these differences impair fertility (and some, like streak gonads, can even cause a high risk of cancer), I would probably call them disorders in most cases.
People who use “they/them” pronouns are often gender nonbinary.
Estrogen (specifically, estradiol) is produced from testosterone through the action of an enzyme called aromatase. And in turn, testosterone is made from progesterone by an enzymatic pathway. So, both males and females make all of these hormones, but at different levels. For more on the biosynthesis pathways of steroid sex hormones, see here. Also, in females, levels of estrogen and progesterone vary during the menstrual cycle, and progesterone levels are much higher in pregnant women. During pregnancy progesterone is produced by both the ovaries and the placenta, and this hormone regulates many aspects of pregnancy.
{kind=link}
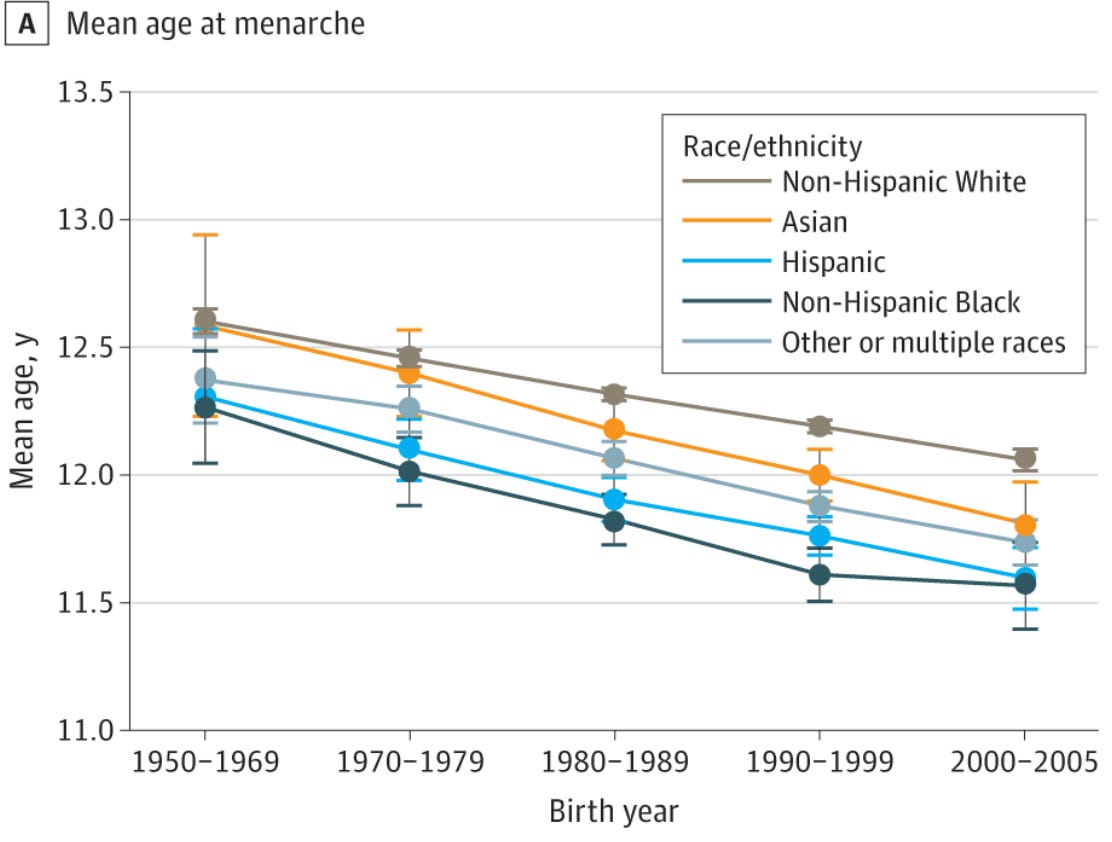
What causes the start of puberty is still an area of research, but it seems that leptin signaling (which relates to body fat percentage) plays a role. The average age of onset of puberty has decreased over the last 150 years and continues to decrease today. Most studies of this have been in girls, since menstruation is a clear-cut marker of female puberty, and the onset of puberty is harder to measure in boys.
In addition to steroid sex hormones, non-steroid hormones such as activin, inhibin, and follistatin are also important here.
In males this is a negative feedback loop. However in females, positive feedback causes large spikes of LH that trigger ovulation during the menstrual cycle. For more information see this review article.
This can also be caused by mutations in regulatory sequences of the SOX9 gene.
They also don’t produce enough cortisol, which causes other problems, but those problems aren’t relevant for this post.
Kallman syndrome also affects non-reproductive biology (like olfaction) but here I’ll just focus on its reproductive effects.
This rate varies among different human populations due different carrier frequencies of certain genetic conditions, and is highest among people originating from southern Africa. Some popular literature has mentioned high intersex rates (up to 1.7%) but these high estimates include “conditions which most clinicians do not recognize as intersex, such as Klinefelter syndrome, Turner syndrome, and late-onset adrenal hyperplasia”.
Historically there were much fewer trans men than trans women, but rates of female-to-male transitions have recently increased to nearly match those of male-to-female transitions.
Although recently rates have increased among the White population faster than other populations.
In New York, 3.0% of youth identify as transgender, whereas in Wyoming 0.6% do (only ~200 individuals). For adults, 0.87% of those in North Carolina identify as transgender whereas 0.20% of those in Missouri do.
Data are not available for youth aged 13-17 but I would expect a similar increase has taken place.
If a trait is genetically heritable, monozygotic (identical) twins should be more similar than dizygotic (fraternal) twins. The degree to which this is true can be used to estimate the genetic heritability.
Defined as the amount of total variation that’s explained by genetic variation.
Alex Jones infamously ranted about “chemicals in the water turning the frogs gay”, but herbicides actually can disrupt sexual development in amphibians. Amphibians are more sensitive than mammals though, because they do their entire development in the water, instead of a more isolated environment like a uterus.
I am not sure this adequately explains why the recent rise is concentrated among young people, though.
The idea of “social contagion” is a sub-category of this latter example that is often the preferred explanation of conservatives.
Conservatives: Medical transition is dangerous and causes bone disease!
Liberals: Transition is proven to be medically safe!
Actual scientific papers: Trans people have weaker bones BEFORE any treatment happens at all. No one knows why. We should probably, like, figure that out or something.
(Citations:
"Low bone mass is prevalent in male-to-female transsexual persons before the start of cross-sex hormonal therapy and gonadectomy", figure 1, page 4:
https://sci-hub.tw/10.1016/j.bone.2013.01.039
Adolescent trans women have average bone density Z-scores of -0.44 SD, -0.77 SD, -0.93 SD, -0.66 SD (depending on metric used) *before* treatment, Table 2:
https://academic.oup.com/jcem/article/100/2/E270/2814818
Z-scores of -0.71 SD, -0.2 SD in young adolescents, and -0.44 SD, -1.18 SD in older adolescents at baseline, Table 2:
https://sci-hub.tw/10.1016/j.bone.2016.11.008
Adult trans women have Z-scores of -0.93 SD, -0.58 SD, -0.73 SD before starting HRT, Table 1:
https://onlinelibrary.wiley.com/doi/full/10.1002/jbmr.3612)
I know yours is not a genetics or medicine Substack, but I passed by and needed to comment on 'causes': Transgender women were gestated in the womb as physically female initially, for any period of time (typically brief), then a genetic mutation (that is caused by a virus that we typically know as a virus that causes the symptoms of UTIs, which also causes CAH) causes a switch in 'sex' to physically male. They are then born as male despite having a deep biological memory of having been inseminated and gestated as female and of developing as girls. It's a manmade bioweapon targeting gay women.
XX individuals switch to XXY and back (for sperm production) during their lives (it's speculated that it is to produce spermatozoa, which come from the Skene glands) and XXY is not an anomaly; XX and XXY chromosomes are both present in all AFAB people. But perhaps the bigger story there is that women produce sperm and always have.