

Base editing, coming soon to a liver near you

Yesterday, an exciting new paper was published,1 which showed that CRISPR base editing can permanently lower LDL cholesterol levels in monkeys.2 Let’s take a look at what the researchers did, and what would be required to do this in humans.
The Target: PCSK9
In order to lower LDL levels, the researchers disabled the PCSK9 gene, which codes for the PCSK9 protein. This protein inactivates LDL receptors on the surface of cells, which are involved in removing LDL cholesterol from the blood. Humans with abnormally high levels of PCSK9 have abnormally high cholesterol, and are predisposed to coronary artery disease. Interestingly, there are a few known human cases where PCSK9 is naturally inactive due to mutation. These people have unusually low LDL levels, and are protected from coronary artery disease.3
Therefore, disabling PCSK9 was hypothesized to lower LDL levels. This has successfully been accomplished in humans through monoclonal antibody treatment,4 where antibodies bind to PCSK9 and inhibit its function. However, monoclonal antibodies are relatively expensive and are not a permanent treatment. Gene editing is a promising alternative. PCSK9 editing was first tested in mice in 2014, with successful results.5
As an additional note, PCSK9 is a good target for gene editing because it is mainly expressed in the liver, which is a very easy target to edit. Since the liver acts as a filter for the blood, anything that gets put in the blood will end up in the liver (whether you want it to or not). In this case, this is a good thing.
The Method: Adenine base editing, delivered by mRNA
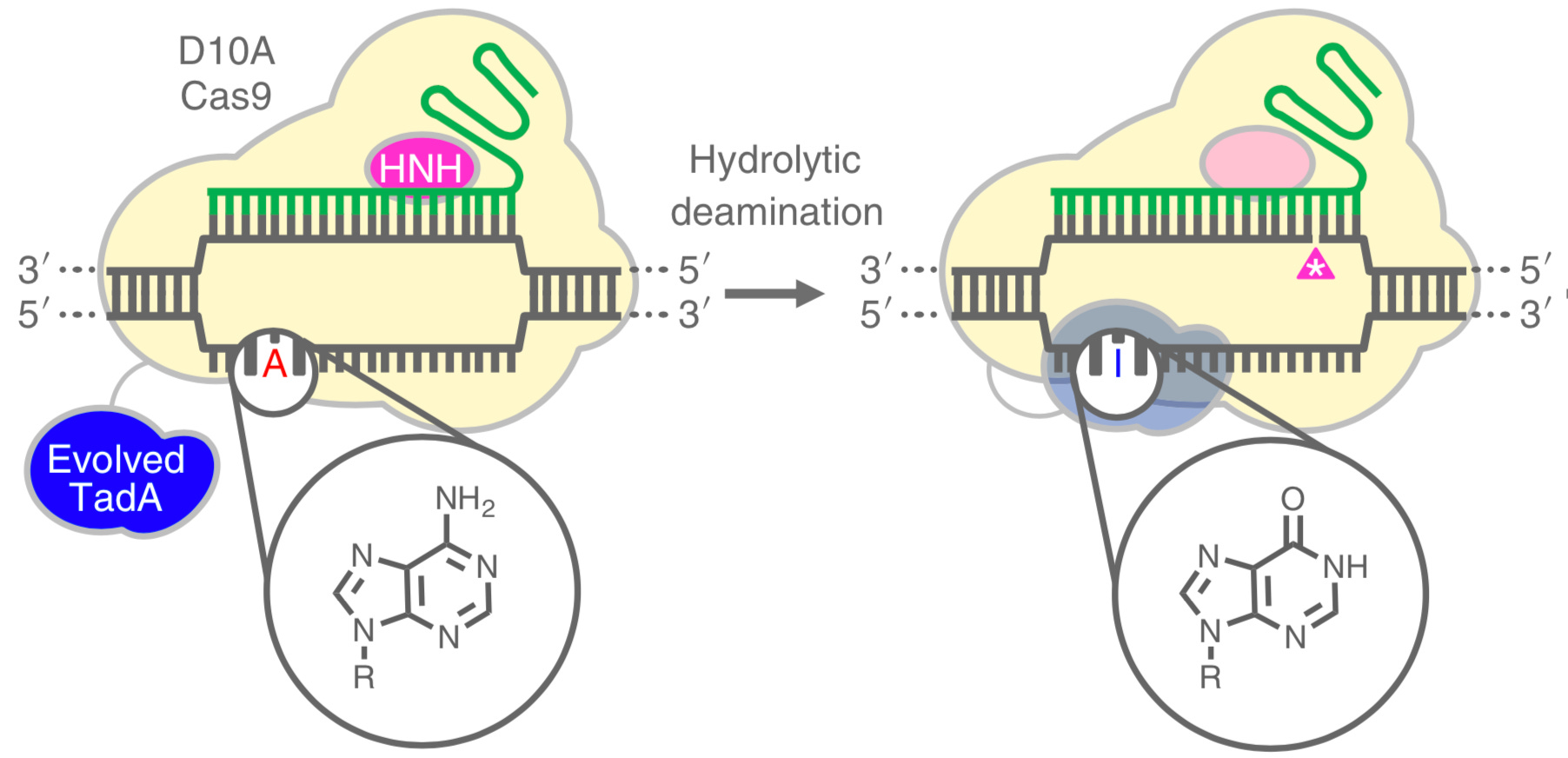
Adenine base editing is a method for converting A (adenine) to G (guanine) at a targeted site in the genome. It works by having an adenosine deaminase attached to a Cas9 variant. Adenosine deaminase is an enzyme which acts on single-stranded DNA and hydrolyzes the amino group on A, converting it to a keto group and thereby changing the base to inosine (I), which is structurally similar to G, and is treated as such by cellular enzymes.6
The Cas9 variant is targeted to the desired site by a guide RNA molecule. Binding of the Cas9 to the target site opens up a short loop of single-stranded DNA, which can then become the substrate for adenosine deaminase. The Cas9 variant is mutated so that it only cuts the non-edited strand of DNA instead of creating a double-strand break (DSB) like normal. This causes the cell to repair the non-edited strand using the edited strand as a template, so both strands become edited.
The main advantage of using base editing, rather than simply cutting the gene to disable it, is safety. Creating double-strand breaks in DNA can cause cell death, and off-target breaks are a much worse problem than off-target base editing. However, base editing does have a disadvantage in that the combined Cas9-deaminase protein is quite large, requiring a long gene to encode it. This is a problem because the most common viral delivery methods (AAVs) cannot fit such a long gene inside them. To get around this, the authors used RNA lipid nanoparticle delivery, with combined delivery of the Cas9-deaminase mRNA and the targeting gRNA. This technology is very similar to what is used in the mRNA COVID-19 vaccines. The target sequence was the exon 1 – intron 1 splice junction in PCSK9. Mutation of an A to a G at this site interrupts RNA splicing and prevents the production of functional PCSK9 protein.
The Results
The researchers first tested a variety of candidate gRNAs on cultured human and cynomolgus monkey hepatocytes, and observed a 60% editing rate with the top one. (The human and monkey target sequences are the same, due to the close relatedness of the two species.) Next, the researchers targeted the homologous site in mouse livers by intravenous injection of the RNA-lipid nanoparticles. Again, the researchers observed efficient editing.
After completing mouse studies, the researchers then moved on to monkeys. They did quite a few measurements of various responses, but the main takeaway is that they observed a ~90% reduction of PCKS9 protein levels, and a ~60% reduction in LDL cholesterol which lasted for at least 8 months (the duration of the study). Off-target editing was minimal, and in fact almost all of the lipid nanoparticles ended up in the liver. A small, temporary increase in liver stress biomarkers was observed, but it was determined to be the result of the lipid component of the nanoparticles, and not the base editing.
What now?
This is all very exciting and I’m optimistic about the possibilities for using this in humans. Given that humans with nonfunctional PCSK9 are known to be healthy, the on-target safety profile seems excellent. Off-target side effects are also likely to not be an issue.
Personally, I’m a healthy person in my mid-20s, and I see no immediate need to lower my LDL levels. But if I were crazy and wanted to try this on myself, here’s what I’d need:
1. The guide RNA.
The target site is listed in their supplementary table 1:
CCCGCACCTTGGCGCAGCGG
with the edited A in bold. The full guide RNA sequence would thus be:
CCCGCACCUUGGCGCAGCGGguuuuagagcuagaaauagcaaguuaaaauaaggcuaguccguuaucaacuugaaaaaguggcaccgagucggugcuuuu
Here the constant region (needed to bind to Cas9) is in lowercase.
I could order this as a chemically synthesized RNA today, with stabilizing modifications, from a lab supplier for around $1000. Smaller quantities would cost less, but for human treatment a few tens of milligrams would be required. (At larger scales, the price per milligram would come down a lot though.)
2. The adenine base editor mRNA.
The researchers used a base editor called ABE8.8-m, the sequence of which is not given in the paper, but it is given in one of their references.7 Fortunately, a plasmid encoding ABE8.8-m is available from Addgene for just $75.8 This is a big help, but it still needs a few more steps to get to the mRNA suitable for delivery. T7 polymerase could be used for in vitro transcription, and the mRNA could then be enzymatically capped for better stability. These processes aren’t trivial, but these days they are pretty straightforward. Estimated cost: around $1000 for one dose
3. The lipids and machine for making nanoparticles
The lipids they used are described in one of their references, and the chemical structures are given.9 They aren’t that difficult to make. Estimated cost: around $1000
Unfortunately the machine for assembling them into nanoparticles is much more expensive. Basically, the lipid and RNA solutions are precisely mixed using microfluidic channels. I can’t even get a quote for such a machine right now (they are all being used to make COVID-19 vaccines). A good summary of the technology is here.
It may be possible to make a bootleg one, but it won’t be easy. On the other hand, the machine would only be required for a short time, so maybe it could be rented? Estimated cost: $1000 – $100,000 depending on how expensive LNP assembly is.
Summary and Conclusions
This paper shows that adenine base editing of PCSK9 can be an effective way to permanently lower LDL cholesterol levels. Safety needs to be demonstrated, but the initial results in monkeys are encouraging. The technology could be applied for humans at a marginal cost of a few thousand dollars. Economies of scale would likely reduce this much further; consider that an mRNA COVID-19 vaccine costs around $15 per dose.10
https://www.nature.com/articles/s41586-021-03534-y
Note on academic references: if you can’t access them, Sci-Hub is your friend.
LDL cholesterol is a cause of coronary artery disease.
https://doi.org/10.1016/j.cell.2019.02.003
https://en.wikipedia.org/wiki/Evolocumab
https://pubmed.ncbi.nlm.nih.gov/24916110/
https://www.nature.com/articles/nature24644 (see especially Figure 1)
https://www.nature.com/articles/s41587-020-0491-6
https://www.addgene.org/136294/
https://doi.org/10.1016/j.celrep.2018.02.014
https://www.bmj.com/content/372/bmj.n281
Considering that you & I are likely to suffer from some form of CVD during our lifetimes considering its omni-prevalence, there is a case for lowering LDL even in a healthy 20-year old. Reduction of CVD risk may scale with LDL almost all the way down, making a strong case for minimizing LDL to the lowest safe level.
Nice post! Maybe, for the sake of the theoretical discussion of course, you could use an extruder to make the liposomes? Basically it consists of two syringes with a filter paper cassette in between. The pore size in the filter determines the size of the liposomes, which are made by pushing a suspension of lipids in buffer (and RNA) back and forth ten or twenty times. The liposomes are seperated by ultra centrifugation, voila, RNA containing liposomes!